Animal experiments demonstrating the anti-aging effects of exchanging young blood plasma for old have been prominent in the last two months. Several groups are saying it’s time to translate their findings into human trials. But I’ve recently learned that others have been doing this for several years. What can we learn from their results to guide the next steps in experimentation?
I had never heard of Grifols, the Spanish pharmaceutical company that is the world’s largest supplier of albumin. Since 2005, Grifols has been quietly funding world leaders in plasma exchange research in humans. Albutein® is their brand-name solution of human albumin.
Last month, the first results of the Grifol’s AMBAR trial were released. (AMBAR stands for Alzheimer’s Modulation By Albumin Replacement). It was a much larger-scale phase 2.5 trial, with 496 subjects recruited from sites in Spain and USA, and treated for 14 months. A single treatment consisted of removing 2.5 to 3 litres of blood (more than half the body’s inventory) and replacing it with Albutein. Patients began with 6 weekly treatments, and thereafter there were 12 monthly smaller plasma replacements (0.7 litres), again with Albutein.
Subjects were evaluated with two standard measures, one of cognitive ability and the other of ability to function independently. Most subjects got worse over the year, as AD is a progressive disease. But treated subjects progressed less than half as fast as sham-treated controls. There was enough variation among individuals that even this strong difference in averages was only marginally statistically significant.
Subjects were categorized as “mild” to “moderate” in their cognitive loss. “Moderate” subjects responded a little better than “mild”, within statistical limits.
In the Conboy paper which I recently reviewed, albumin was considered to be just a passive replacement of proteins that every mammal needs. Albumin was replaced in the blood because when harmful signaling proteins were diluted out of the blood, albumin was removed along with it. The body needs the albumin, while the protein signals were doing damage. Henced they replaced the albumin.
But in AMBAR, albumin is considered an active part of the therapy.
[P]lasma albumin from AD patients is more glycated and nitrotyrosinated than plasma from healthy subjects, reducing its ability to inhibit Aβ aggregation Grifols theorized that replacing AD patients’ albumin with therapeutic-grade albumin should overcome this problem. Further, therapeutic-grade albumin should more effectively bind plasma Aβ and sequester it than plasma albumin from AD patients. Albumin may protect neurons by additional mechanisms, including anti-oxidant and anti-inflammatory activities. [review, referencing this primary source].
In one branch of the AMBAR program, ¼ of subjects also received intravenous immunoglobulin (IVIG). This consists of antibodies which identify challenges to which the immune system can respond. Grifols has a proprietary IG product called Flebogamma®. The AMBAR trial was unable to detect a benefit from IVIG.
Plasma exchange has a long history for treatment of auto-immune disorders. Some of the diseases of old age are related to autoimmunity (e.g., diabetes, arthritis, chronic inflammation). Older persons have a higher generalized autoimmunity, but a lower incidence of explicitly autoimmune diseases. Presumably, there are antibodies to self that accumulate in the bloodstream with age, and in recent years this has been related to leaky gut disorders. It makes sense to me that blood dilution would be a downstream or stop-gap treatment for autoimmunity, but that better approaches would be directed at the source of the offending antibodies.
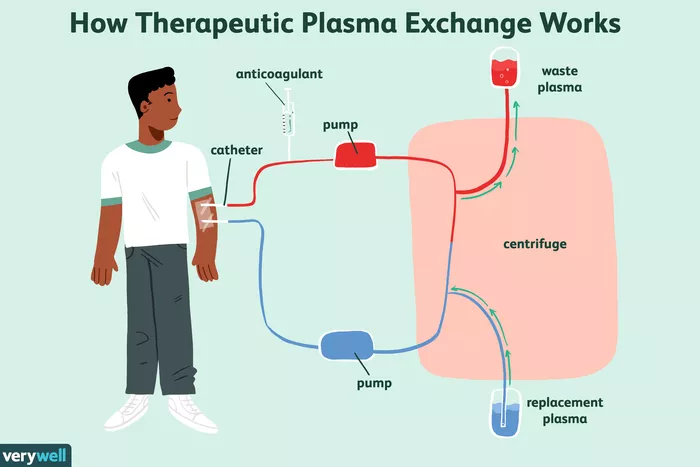
Dobri Kiprov was a co-author of the Conboys’ plasma dilution paper. Kiprov’s clinic has been a site in the AMBAR trials, with experience in plasma exchange going back 20 years. Kripov has studied plasma exchange for a variety of diseases. In these treatments, a patient’s blood is removed and separated. The patient’s own red and white blood are returned to him, but his plasma is replace with saline, albumin, and possibly other ingredients. When I spoke to him, he described work which is soon to be published in Alzheimer’s and Dementia involving a proprietary added ingredient in these plasma transfusions. Benefits last at least 6 months, he said, which suggests that there is some epigenetic re-programming of the cellular sources of blood constituents.
Kiprov claims that patients who receive frozen blood plasma for a variety of reasons have fewer adverse reactions when they receive plasma from young donors (18-24) compared to middle-aged donors (35-45). He has seen patients’ immune systems improve, and arthritis symptoms decrease. He’s eager to see formal trials proceed for these conditions (but someone has to fund them).
The bottom line
As a treatment for AD, these results are not impressive. Patients were already quite disabled, and the results were essentially to prolong their end-of-life institutional existence. There are no effective drugs for AD, so compared to any pharmaceutical, AMBAR looks good. But compare these results to Bredesen’s RECODE program, which aims to improve cognition, and in some cases has returned people to productivity from a non-functional state. RECODE works better the earlier you start it, whereas preliminary results suggests that AMBAR is more effective in late stages.
Inflammation is a driver of all the diseases of old age. Pro-inflammatory signals (cytokines) in the blood were among the elements diluted by AMBAR, and it may be that reduction in inflammation fully accounts for the program’s successes.
As a proof of principle, the results are quite informative. A benefit was demonstrated from plasma exchange in humans for the first time. Subjects did not become dramatically younger, despite much more dilution than in the Conboy mouse experiments (reviewed in this space earlier this month). They suggest that simple dilution as pioneered by the Conboys in mice might be effective in slowing senescence but not reducing biological age.
Two plasma exchange doctors were kind enough to help me with this column. I’m grateful to David Haase (TX) and Dobri Kiprov (CA) for offering background and providing direction to my readings.