Gender-affirming facial surgery (GFS) is pursued by transgender individuals who desire facial features that better reflect their gender identity. Until now, there have been few objective guidelines to justify and facilitate effective surgical decision-making for gender-affirming facial surgery.
In order to validate surgical decisions for GFS, researchers from the UC San Francisco and the University of Calgary set out to quantify the effect of sex on adult facial size and shape through an analysis of three-dimensional (3D) facial surface images.
In a study published online this week in Facial Plastic Surgery & Aesthetic Medicine, the investigators undertook a surgically oriented analysis of 3D facial size and shape to quantify and visualize facial sex differences. Their findings reveal significant differences in both shape and size of male and female craniofacial features and provide data-driven anatomic guidance and justification for GFS, particularly for forehead contouring cranioplasty, mandible and chin alterations, rhinoplasty, and cheek modifications.
“Our purpose was to establish an important, definitive, and biologically-based relationship of facial features to sex. This empowers the patient to navigate towards a facial appearance that matches with their gender identity, and thereby reduces mis-gendering and gender dysphoria while improving self-perception,” said senior author Rahul Seth, MD, Associate Professor in the Facial Plastic and Aesthetic Surgery in the UCSF Department of Otolaryngology-Head and Neck Surgery. “We feel that this data provides surgeons, patients, and insurance payors with a life-like and surgically-oriented analysis of 3D facial size and shape to guide patients and surgeons in performing these complex and life-altering surgeries.”
Brow, Jaw, Nose, Cheek Show Biggest Differences by Sex
The researchers were able to determine that, on average, male faces are 7.3% larger than female faces. Sex was associated with significant facial shape differences in the entire face as well as in each sub-region considered in the study. The facial regions in which sex has the largest effect on shape are the brow, jaw, nose, and cheek. The authors, therefore, provide supportive evidence and guidelines for the appropriate alterations of these facial areas for GFS, although each individual patient’s goals and face is unique.
To yield these results, the researchers obtained facial measurements by applying an atlas facial surface to 3D surface scans of 545 males and 1028 females older than 20 years of age. The differences between male and female faces were analyzed and visualized for a set of predefined surgically relevant facial regions.
Each scan used a 3D surface mesh comprised of 3D vertices connected by triangles. The triangular meshes were used to digitally represent surface data. While the exact number per face differed slightly in the raw data, each mesh contained 27,903 vertices to provide consistent, high-resolution facial data. Concepts central to rigorous geometric morphometrics were applied to the surface data to provide detailed results.
To analyze the effects of sex on facial size and shape, a variety of facial sub-regions were first specified based on the potential for surgical application and relevance to surgical decision making and planning. The regions included both large area sections of the face (cheeks, nose) as well as axial or sagittal curves. Dense surface-based measurements and comparisons of form, size, and shape were performed for the whole face and facial subregions.
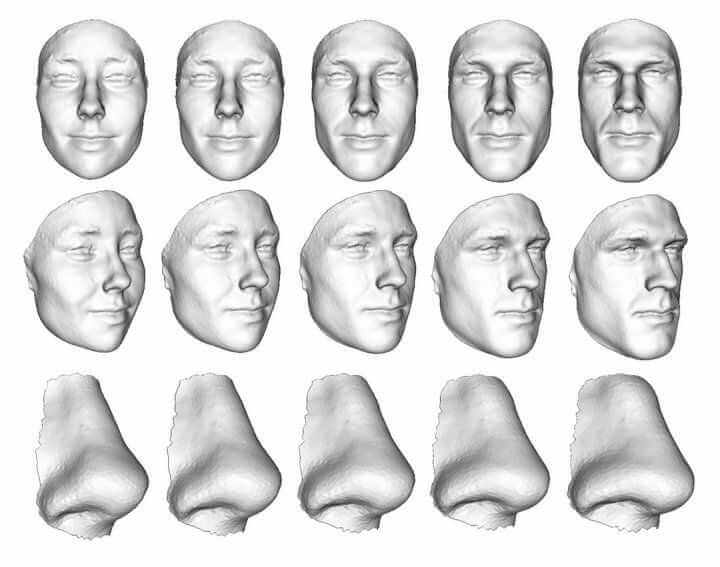
The researchers represented their findings in a “heat map” to show the mean difference between male and female facial shape differences. Using this information, these changes were applied to an example face to demonstrate their validity to “surgically” alter the face along an axis of masculinity and femininity.
While the study provides important differentiators for male and female facial size and shape differences, the results also suggest that in some cases, effective gender modification may be achieved by over-correcting either size or shape. For example, if functional concerns prevent a surgeon from reducing jaw size, it may be most ideal to contour the area to be less square, emphasizing a more feminine shape.
The findings of this study provide anatomic rationale and guidance that may enable optimal GFS results for transgender and gender diverse individuals.
Authors: First author is Jordan Bannister, BASc, University of Calgary, Biomedical Engineering Graduate Program. Co-Authors are Hailey M. Juszczak, BA, and P. Daniel Knott, MD, UCSF, Division of Facial Plastic and Reconstructive Surgery, Department of Otolaryngology-Head and Neck Surgery; J. David Aponte, MSc, David C. Katz, PhD, and Benedikt Hallgrimsson, PhD, Department of Cell Biology and Anatomy, Alberta Children’s Hospital Research Institute, University of Calgary; Seth Weinberg, University of Pittsburgh, Department of Oral and Craniofacial Sciences, School of Dental Medicine; Nils D. Forkert, PhD, University of Calgary, Department of Radiology, Alberta Children’s Hospital Research Institute and Hotchkiss Brain Institute, Cumming School of Medicine.
Funding: This research was funded by the of and the National Institutes of Health (U01-DE024440) and the Canada Research Chairs program.
Disclosures: Authors J.J.B., J.D.A, D.C.K., B.H., N.D.F., and R.S. are affiliated with Deep Surface AI, Inc., a company specializing in 3D facial analytics and morphing.
If our reporting has informed or inspired you, please consider making a donation. Every contribution, no matter the size, empowers us to continue delivering accurate, engaging, and trustworthy science and medical news. Independent journalism requires time, effort, and resources—your support ensures we can keep uncovering the stories that matter most to you.
Join us in making knowledge accessible and impactful. Thank you for standing with us!