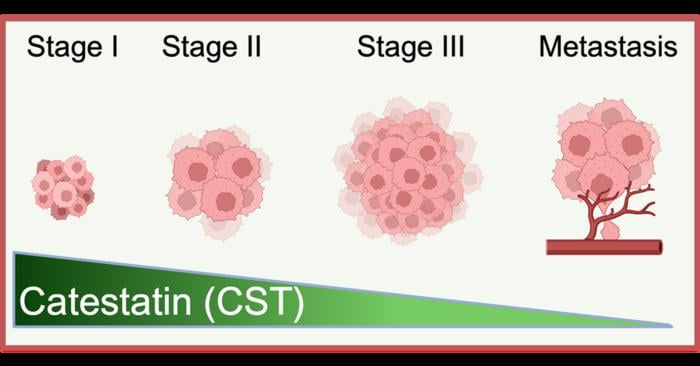
Somewhere inside your skin right now, a small protein fragment is going about its business. It helps regulate inflammation. It assists in wound repair. And, it turns out, it may be quietly suppressing the kind of cellular chaos that leads to melanoma. The molecule is called catestatin, and until very recently nobody had thought to look at what happens to it in skin cancer. When researchers at UC San Diego finally did, they found something that felt like a clue: as melanoma progresses to more aggressive stages, catestatin levels fall. Consistently, in patient after patient.
The implication, if it holds up, is unsettling in a specific way. The body, it seems, may already know how to fight this cancer. The tumor learns to silence the defence.
Catestatin is derived from a larger protein called Chromogranin A, or CgA, which you’ve probably never heard of but which does rather a lot. CgA is involved in cardiovascular regulation, immune signalling, metabolic control, neuroendocrine communication; it’s one of those proteins that turns up everywhere once you start looking, which is perhaps why the peptide fragment it produces has taken so long to attract serious oncological attention. Researchers had studied catestatin’s role in blood pressure, in inflammation, in the strange physiology of stress response. Cancer? Not so much.
Sushil K. Mahata, a professor of medicine at UC San Diego and research physiologist at the VA San Diego Healthcare System, changed that. His team noticed that catestatin appeared in skin tissue and began asking what it might be doing there, specifically in the context of melanoma. What followed was the kind of experimental cascade where each answer generates three more questions.
When the researchers restored catestatin to patient-derived melanoma cells in the laboratory, the cells responded in ways that were, frankly, striking. They began dying off, through a controlled process called apoptosis. They stopped proliferating at their usual rate. They became less invasive, less inclined to migrate in the way that metastatic cancer cells do. And normal skin fibroblasts, sitting in the same experimental environment, were essentially unaffected. The peptide, in other words, appeared to be selectively toxic to the tumour cells and not to healthy tissue around them.
“Melanoma is particularly dangerous because tumor cells can adapt and become resistant to therapy. Our research shows that CST can disrupt those resistance pathways and push melanoma cells back toward a more treatable state,” said Mahata.
That last part, about resistance, is perhaps where the findings get genuinely interesting from a clinical standpoint. Drug resistance is the reason melanoma kills. Vemurafenib, a targeted therapy that works by blocking a mutated version of a protein called BRAF, can be spectacularly effective at first. Then, often within months, the cancer finds its way around it; the cells activate alternative survival routes, upregulate stress-response genes, remodel the extracellular matrix around them to create a more favourable microenvironment. What catestatin appears to do, at least in Vemurafenib-resistant cell lines in the lab, is switch some of those routes off. Transcriptomic profiling showed downregulation of genes involved in hypoxia signalling, in the epithelial-to-mesenchymal transition that helps cancers spread, in the molecular machinery of stress adaptation. Several specific mediators, including proteins involved in extracellular-matrix remodelling and growth factor signalling, were also suppressed. It’s a broad sweep, which is either encouraging or complicated depending on how you look at it.
In mouse models, the results translated reasonably well. Animals given catestatin showed significantly reduced tumour growth and lower overall tumour burden, with no detectable systemic toxicity. Rough numbers, yes, and mouse models are notoriously imperfect proxies for human cancer. But no toxicity is, at minimum, a decent place to start.
Satadeepa Kal, the postdoctoral researcher who led the study, pointed to something that feels worth sitting with. “In the era of small-molecule inhibitors and immunotherapy, the therapeutic potential of peptides remains relatively underexplored,” she said. “Our work demonstrates that peptide-based therapies may offer a powerful strategy not only against melanoma and drug resistance, but potentially against other cancers and complex metabolic diseases as well.” Peptides occupy a peculiar middle ground in pharmacology: more specific than traditional chemotherapy (which has a tendency to rough up everything that’s dividing fast), more targetable than many small molecules, but historically difficult to manufacture and deliver reliably. The field has been inching forward for years.
There are, obviously, caveats. Lots of them. The distance between a promising result in cell lines and mouse models and an actual clinical therapy is usually measured in years, sometimes decades, and many candidates fail to cross it at all. Whether catestatin can be engineered into a stable, deliverable drug that maintains its selectivity in the far messier environment of a human tumour is still an open question. The researchers acknowledge that additional preclinical work and eventually clinical trials will be needed before any of this reaches patients.
What the study does establish, though, is a mechanism worth pursuing. Melanoma kills roughly 8,000 Americans a year, and the proportion of those deaths attributable to therapy-resistant disease is growing as patients who initially respond to targeted treatment eventually relapse. Anything that might restore sensitivity in those cells, or slow the tumour’s adaptation to begin with, has a plausible role in treatment. The catestatin story adds something else to that picture: the suggestion that the body was already trying to suppress the cancer, with a molecule it produces naturally, and that the cancer’s first order of business is to disable that protection.
Whether future therapies will work by supplementing catestatin, or by figuring out why its levels drop and trying to prevent that, or by mimicking its effects through some other molecular route, remains to be seen. The question of how the tumour silences it in the first place hasn’t been answered yet. Which is, probably, the next thing to look at.
https://doi.org/10.1038/s41389-026-00628-y
Frequently Asked Questions
Why does melanoma become resistant to treatment, and could catestatin actually fix that?
Melanoma cells are unusually adaptable; when targeted drugs like Vemurafenib block one survival pathway, the cells activate alternative routes within months, remodelling their molecular environment to stay alive. Catestatin appears to interfere with several of those resistance mechanisms simultaneously, switching off genes involved in stress adaptation, matrix remodelling, and tumour spread. Whether that effect holds in human patients, rather than laboratory cell lines, is the central question the researchers now need to answer.
If the body already makes catestatin, why isn’t it protecting people from melanoma naturally?
This is exactly what makes the finding interesting: catestatin levels decline as melanoma advances, which suggests the tumour is somehow disabling its own natural suppressor. Exactly how the cancer achieves this, whether by silencing the gene that produces Chromogranin A, by degrading the peptide, or by some other mechanism, hasn’t been established yet. Answering that question could open up a second line of attack entirely.
What makes a peptide-based cancer therapy different from chemotherapy or immunotherapy?
Chemotherapy broadly targets rapidly dividing cells, which is effective but hard on healthy tissue. Immunotherapy recruits the immune system, which can be powerful but unpredictable. Peptides like catestatin sit in a different category: they can be designed to interact with specific molecular pathways, potentially hitting tumour cells while leaving normal tissue largely alone. The UC San Diego study found exactly that kind of selectivity, with melanoma cells dying while adjacent healthy fibroblasts were unaffected.
How far is catestatin from being an actual drug people could use?
Several years at a minimum, and potentially much longer. The current results come from cell cultures and mouse models, which are useful starting points but often don’t translate cleanly to humans. Before clinical trials could begin, researchers would need to establish how to deliver the peptide reliably, confirm it maintains its selectivity in a human tumour environment, and demonstrate safety at therapeutic doses. The pathway is credible; the timeline is not yet knowable.
ScienceBlog.com has no paywalls, no sponsored content, and no agenda beyond getting the science right. Every story here is written to inform, not to impress an advertiser or push a point of view.
Good science journalism takes time — reading the papers, checking the claims, finding researchers who can put findings in context. We do that work because we think it matters.
If you find this site useful, consider supporting it with a donation. Even a few dollars a month helps keep the coverage independent and free for everyone.