Start with a number that ought to give the whole boom pause: within a year of starting one of the new weight-loss injections, roughly two-thirds of people taking them for obesity alone have stopped. Sixty-five percent, give or take. The drugs work, spectacularly in many cases, and then a great many people simply put them down, and the weight, more often than not, comes back. That is the awkward shadow sitting behind the semaglutide and tirzepatide story everyone has been telling.
It is also the starting point for a new commentary in the journal Gastroenterology, the official journal of the American Gastroenterological Association. The paper, titled “Revisiting POWER in the GLP-1 Age,” is essentially a stocktake: what has actually changed in obesity medicine since 2017, and what to do about it.
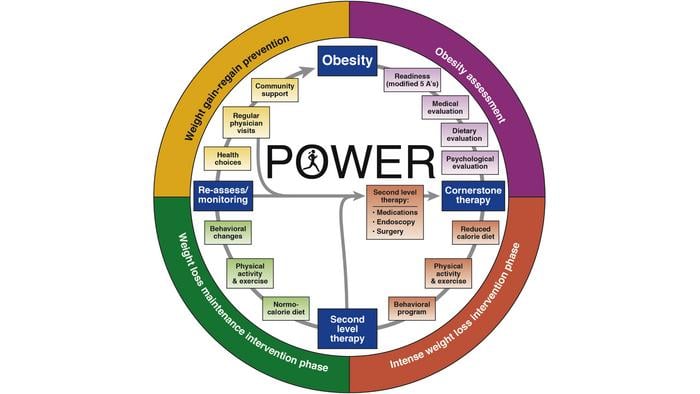
That year, 2017, the association published something called POWER, a practice guide meant to give physicians a structured, multidisciplinary way to treat obesity rather than the usual eat-less-move-more shrug. Then the GLP-1 drugs arrived and rearranged the furniture. Ozempic and Wegovy (both semaglutide), Zepbound and Mounjaro (tirzepatide): names that have leaked out of clinics and into ordinary conversation. The authors set out to update the old framework for a world where these medicines exist. Hence POWER 2.0, which they describe, a touch optimistically perhaps, as a live document.
Here is the thing the headlines tend to skip. The injections are genuinely good at what they do.
Across the trials, this class of drug has reliably pushed people past the 10 percent total-body-weight-loss mark, the rough threshold where the knock-on conditions, the diabetes, the high blood pressure, the sleep apnoea, the fatty liver, start to ease as well. That is not a small thing. For a long stretch of medical history nothing short of surgery could do it.
The Catch Nobody Wants on the Billboard
But the discontinuation figures are stubborn, and they vary in a revealing way. People taking the drugs for obesity alone quit at around 64.8 percent inside twelve months; for those with type 2 diabetes alone the rate drops to 46.5 percent; for people with both, down again to 34.2 percent. Stop, and weight regain tends to follow, along with the metabolic problems that came with it. There is cost, too. One independent review judged the new class poor value compared with the older, cheaper anti-obesity drugs, and the Congressional Budget Office has forecast something like an extra $35 billion in federal spending on these medications between 2026 and 2034. Effective, yes. Cheap and self-sustaining, not exactly.
So the commentary’s argument, and it is one worth sitting with, is that the drug on its own is a tool, not a cure, and that obesity is better understood as a chronic, relapsing disease than as a number on a scale to be knocked down once. The authors lean on a recent idea from a Lancet commission called “clinical obesity,” meaning obesity that is already doing organ-level harm, and they push back on the old habit of reading body mass index as the whole story. BMI plus waist circumference, they suggest, tells you rather more than BMI alone.
Which is where the gastroenterologists come in, because the paper is in their journal and is, in part, a pitch to their own specialty. They are the doctors already seeing the downstream wreckage of obesity: reflux, gallbladder disease, the fatty-liver condition now abbreviated MASLD. And they have tools of their own that the injection conversation tends to forget. Take endoscopic sleeve gastroplasty, ESG for short, a procedure in which a doctor threads a suturing device down through the mouth and stitches the stomach smaller from the inside, no incision required. In the MERIT trial, 209 patients who had the procedure lost about 13.6 percent of their body weight at one year against 0.8 percent in the control group, and held on to more than 80 percent of that loss at two years. Serious complications ran to roughly 2 percent. Intragastric balloons, swallowed or placed and later removed, sit further down the same menu, and full bariatric surgery, still the most durable option of all, sits at the bottom with a perioperative mortality of about 0.1 percent, lower, the authors point out, than a routine gallbladder removal.
Mixing the Toolkit Rather Than Picking a Side
What seems to genuinely interest the authors, though, is not any single tool but the act of combining them. As the commentary puts it, combining GLP-1 medications with endoscopic or surgical interventions may produce greater and more durable weight loss than either approach alone. The numbers back the instinct, at least early on: one study pairing ESG with the older drug liraglutide reported about 24.7 percent total body weight loss at a year, well beyond what the procedure managed by itself. And there are early gestures toward something more personalised still. In one trial, people who felt full only after eating a lot, high “calories to satiation,” in the jargon, did best on one drug combination, while the easily sated did better on another. Match the patient to the mechanism, in other words, rather than handing everyone the same prescription and hoping.
None of this is settled, and the commentary is honest enough about the gaps. The combination data are still thin, follow-up is short, and reimbursement, that quiet killer of good ideas, has long kept the endoscopic procedures out of reach for many patients (a new billing code, the authors note, may finally start to loosen that). And the disease keeps spreading downward in age: severe obesity in American children climbed from 4.9 percent around the turn of the century to 7.6 percent by the late 2010s, a trend no injection alone is going to reverse.
What the paper is really describing, then, is less a breakthrough than a correction. The drugs did not end the obesity story; they opened a louder chapter of it, and somewhere in the excitement the older, less glamorous truth, that lasting change in a chronic disease usually takes a team, a plan, and more than one lever, got a bit drowned out. The clinic of the near future, on this reading, looks less like a pharmacy counter and more like a workshop: a drug here, a stitched stomach there, a dietitian and a behavioural specialist somewhere in the room, all aimed at the same body. Whether health systems will pay for that fuller picture, rather than just the prescription, is the open question.
For now the lesson is almost old-fashioned, dressed in very new clothes. The miracle, it turns out, still needs a follow-up appointment.
Source: Revisiting POWER in the GLP-1 Age, Gastroenterology (2026)
Frequently Asked Questions
If GLP-1 drugs work so well, why do doctors say they aren’t enough on their own?
Because the results often don’t last once the injections stop. Within a year, most people taking these drugs for obesity alone discontinue them, and weight regain usually follows, along with the conditions that came with it. The argument in the new commentary is that obesity behaves like a chronic, relapsing disease, so treating it well tends to mean a sustained plan rather than a single fix.
What is endoscopic sleeve gastroplasty, and how is it different from weight-loss surgery?
It is a procedure where a doctor passes a suturing device down through the mouth and stitches the stomach into a smaller shape from the inside, with no surgical incision. In one major trial, patients lost about 13.6 percent of their body weight at a year and kept most of it at two years, with serious complications in roughly 2 percent of cases. It sits between drugs and full bariatric surgery on the scale of how invasive and how durable these options are.
Is it true that combining a weight-loss drug with a procedure works better than either alone?
Early evidence points that way. One study that paired endoscopic stomach stitching with an older weight-loss drug reported substantially more weight loss at a year than the procedure managed by itself. The data are still limited and the follow-up short, so the size of the long-term advantage isn’t yet clear.
Why does the move away from BMI matter for ordinary patients?
Body mass index doesn’t distinguish well between weight that is harming someone and weight that isn’t, especially at the individual level. The newer idea of “clinical obesity” focuses on whether excess fat is actually damaging organs, and pairs BMI with measures like waist circumference for a clearer read. For patients, that can mean treatment decisions based on real health risk rather than a single number on a chart.
ScienceBlog.com has no paywalls, no sponsored content, and no agenda beyond getting the science right. Every story here is written to inform, not to impress an advertiser or push a point of view.
Good science journalism takes time — reading the papers, checking the claims, finding researchers who can put findings in context. We do that work because we think it matters.
If you find this site useful, consider supporting it with a donation. Even a few dollars a month helps keep the coverage independent and free for everyone.