A quiet threat may lurk inside our arteries. Researchers from Tampere University, Oulu University, and the University of Oxford report that bacterial biofilms, long thought harmless passengers, may in fact trigger myocardial infarction.
Published in the Journal of the American Heart Association, the study suggests heart attacks could sometimes be infectious in origin, a finding that rattles decades of cardiovascular dogma and points toward new diagnostics, treatments, and even vaccines.
Coronary plaques, once believed to form solely through oxidized LDL cholesterol and inflammation, were found to harbor bacterial DNA—especially from oral viridans streptococci—in more than 40 percent of autopsied and surgical samples. These bacteria assemble into biofilms, slimy fortresses that antibiotics and immune cells cannot penetrate. When activated, the biofilm sheds virulent bacteria into the arterial wall. The immune system detects the invaders too late, igniting inflammation that ruptures the plaque and unleashes a fatal clot.
From Suspicion to Evidence
Cardiologists have debated an infection link to heart disease since the 1980s, but proof was thin. This time, researchers combined bacterial DNA analysis, immunohistochemistry, and gene expression studies on tissue from 121 sudden cardiac death victims and 96 surgical patients. The results were consistent: biofilms were not innocent bystanders. They were embedded in advanced plaques and directly associated with myocardial infarction.
“Bacterial involvement in coronary artery disease has long been suspected, but direct and convincing evidence has been lacking,” said study leader Professor Pekka Karhunen of Tampere University (JAHA).
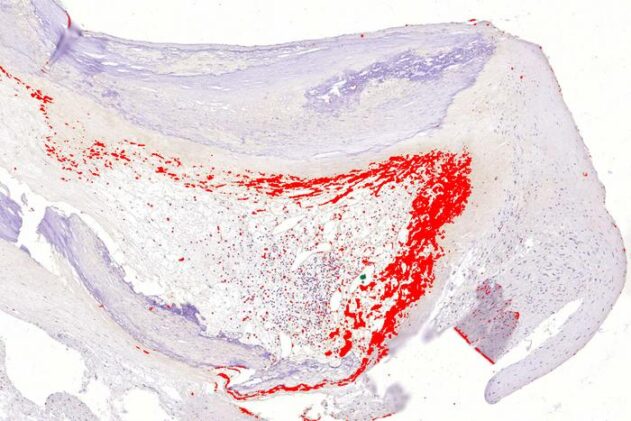
Immunostaining revealed thick mats of streptococcal biofilm inside plaques, invisible to macrophages. When ruptures occurred, scattered bacteria appeared at the fibrous cap, engaging the immune system’s toll-like receptors (TLR2 especially) and triggering inflammatory cascades. Genome-wide expression analysis confirmed upregulated bacterial recognition pathways, strengthening the case that biofilms are not passive debris but active instigators.
Key Findings
- DNA from viridans streptococci was found in 42% of coronary plaques and 43% of surgical endarterectomy samples.
- Biofilms evaded innate immune detection but released virulent bacteria at rupture sites, detected by toll-like receptor signaling.
- Immunopositivity strongly correlated with severe atherosclerosis and with death from myocardial infarction.
- Genome-wide analysis showed bacterial recognition pathways were highly upregulated in diseased arteries.
Implications for Prevention and Care
This infection hypothesis could explain why past antibiotic trials targeting single pathogens, like Chlamydia pneumoniae, largely failed. Biofilms resist most drugs, and plaque rupture might be sparked by external triggers—respiratory infections, stress hormones, even seasonal influenza. It aligns with epidemiological data showing heart attack risk spikes during flu season (CDC).
“Our study demonstrated the presence of genetic material—DNA—from several oral bacteria inside atherosclerotic plaques,” Karhunen said.
If coronary disease is partly infectious, it opens radical possibilities: vaccines against oral bacteria, new imaging tools for detecting biofilms, and short-term antibiotic or anti-biofilm therapies during acute infection. Public health messaging may one day treat dental care not only as hygiene, but as cardiovascular prevention.
Takeaway
The Finnish-UK team’s findings suggest that hidden bacterial biofilms in arterial plaques can spark fatal heart attacks when activated. The work reframes myocardial infarction as not only metabolic and inflammatory, but potentially infectious—a shift that could inspire new vaccines, diagnostics, and therapies targeting biofilms.
Journal: Journal of the American Heart Association
DOI: 10.1161/JAHA.125.041521
ScienceBlog.com has no paywalls, no sponsored content, and no agenda beyond getting the science right. Every story here is written to inform, not to impress an advertiser or push a point of view.
Good science journalism takes time — reading the papers, checking the claims, finding researchers who can put findings in context. We do that work because we think it matters.
If you find this site useful, consider supporting it with a donation. Even a few dollars a month helps keep the coverage independent and free for everyone.