Key Takeaways
- Choline acetyltransferase manufactures acetylcholine, traditionally linked to the nervous system but now found in immune cells like T cells and B cells.
- Research reveals a ‘shadow nervous system’ within the immune system, using neurotransmitters like acetylcholine, dopamine, and GABA to communicate and regulate responses.
- Context-dependency of neurotransmitter effects complicates therapeutic targeting, as the same molecule can yield opposite outcomes based on its source and tissue environment.
- Emerging studies suggest antidepressants and other drugs might enhance immune responses by modulating neurotransmitter pathways.
- Further research aims to unravel the complex relationship between the immune and nervous systems, potentially leading to novel treatment strategies.
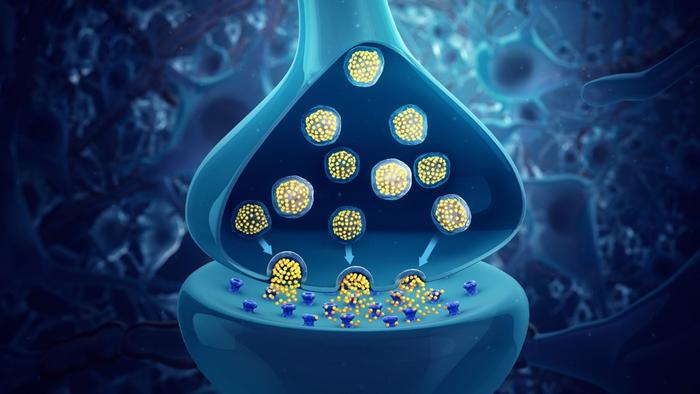
Choline acetyltransferase is an enzyme with one job: manufacturing acetylcholine. For most of the twentieth century, that job was considered strictly neurological. The enzyme lives in neurons. Neurons release acetylcholine. Acetylcholine tells your heart to slow down, your pupils to contract, your gut to keep moving. The whole system has a name, the parasympathetic nervous system, and it is exquisitely mapped; researchers know its anatomy down to individual nerve fibers in specific organs. The spleen, notably, has no parasympathetic innervation at all. And yet, when scientists began looking carefully, they found acetylcholine there anyway.
Something else was making it. T cells, as it turned out. B cells too. Natural killer cells. Even macrophages.
That discovery, confirmed across a run of studies through the 2010s and accelerating sharply in the years since, has forced a rethinking of what immune cells actually do. A review published in March 2026 in the journal Immunity & Inflammation, from researchers at the University of Hong Kong, maps the full scope of what is now emerging as a kind of shadow nervous system within the immune system itself, one that speaks in the same chemical language as neurons but operates according to its own rules, with consequences for autoimmune disease, cancer, and infection that researchers are only beginning to untangle.
The chemicals involved are ones you probably associate entirely with the brain. Acetylcholine, the “rest-and-digest” transmitter. Dopamine, the molecule of reward and anticipation. Norepinephrine (noradrenaline), the stress hormone that also mediates the sympathetic fight-or-flight response. GABA, the brain’s primary brake signal. Serotonin, better known for its role in mood. Histamine, famous for allergies. These are textbook neurotransmitters, the chemicals of synapses and signaling speed and millisecond-scale communication between neurons. The idea that white blood cells are producing them, storing them in vesicles, and releasing them to communicate with neighboring cells in the lymph node or the tumor microenvironment or the infected lung, still carries a faint whiff of the implausible. The evidence, however, has become hard to argue with.
What makes the system particularly strange, and clinically significant, is a property the Hong Kong researchers call functional pleiotropy. “The same neurotransmitter can exert opposing effects depending on cellular source and tissue context,” the authors write. This is not the kind of thing you want from a drug target. A molecule that suppresses inflammation in the spleen while promoting it in the synovial joint, that helps clear a lung infection while simultaneously slowing the immune attack on a tumor, is going to be extremely difficult to manipulate therapeutically without collateral damage. It is also, in a way, the most interesting thing about the whole field.
Take acetylcholine produced by T cells. In 2011, a landmark paper by Rosas-Ballina and colleagues showed that ChAT-expressing T cells in the spleen relay anti-inflammatory signals through the vagus nerve circuit, essentially acting as a communication node between the nervous system and the immune response. That paper opened a research programme that has since traced acetylcholine-producing T cells into the tumor microenvironment, where certain subtypes, including regulatory T cells and exhausted CD4 cells, suppress the immune attack on liver cancer. Elsewhere, Th17 cells that express the same enzyme appear to worsen experimental autoimmune encephalomyelitis, an animal model of multiple sclerosis. Same molecule. Same immune lineage, broadly speaking. Opposing outcomes.
Yes, and the evidence is now substantial. Multiple immune cell types, including T cells, B cells, macrophages, and dendritic cells, express the enzymes needed to synthesize classic neurotransmitters including acetylcholine, dopamine, norepinephrine, GABA, and serotonin. The discovery upended the assumption that neurotransmitter production was exclusive to neurons, and is now recognized as a major mechanism by which the immune system regulates itself locally, without needing to wait for neural input.
Because the same molecule can do completely different things depending on its source and the local environment. Acetylcholine from B cells promotes liver regeneration after injury, but acetylcholine from certain T cell subsets worsens autoimmune disease in animal models. The effect depends on which receptors are expressed on neighboring cells, what concentration of the signal is present, and what other signaling is happening in that tissue at that moment. This context-dependency is the central challenge in turning the science into treatments.
There is early evidence that they might, in specific contexts. Research published in 2025 found that serotonin transporter inhibitors (SSRIs) enhanced the tumor-killing ability of CD8 T cells by preventing the transporter from sequestering serotonin and suppressing immune function. Preclinical data suggest SSRIs may work synergistically with immune checkpoint inhibitors in several cancer types. Whether this translates reliably into clinical benefit is still being established, but the biological rationale is now clear enough that trials are underway.
The same receptors that appear on immune cells also appear on neurons, cancer cells, and other tissues throughout the body, meaning a drug targeting a dopamine receptor, say, will not discriminate between its effects on T cells and its effects on the brain or gut. This receptor promiscuity is the main obstacle to translating neuroimmune discoveries into clinical use. More targeted delivery strategies, such as antibody-drug conjugates that direct agents to specific immune populations, are being explored, but represent a significant engineering challenge.
B cells complicate the picture further. They are, it turns out, one of the major sources of acetylcholine in the bone marrow, where the neurotransmitter suppresses hematopoietic stem cell proliferation and reduces the production of myeloid cells. That finding has implications for cardiovascular disease and inflammation. In the lung, cholinergic B cells limit inflammatory tissue damage during viral infection; in the liver, they promote regeneration after injury by modulating Kupffer cell function. In skin, acetylcholine from B cells modulates keratinocyte proliferation and reduces pathological thickening. The same cells, the same molecule, acting as a local tissue manager in three different organs in three different ways.
Dopamine’s immunological story is similarly layered. Its synthesis machinery, the enzyme tyrosine hydroxylase, is expressed in T cells, B cells, macrophages and dendritic cells. Follicular helper T cells contain dopamine-storing granules and release substantial amounts during their interactions with B cells in germinal centers; this dopamine signaling appears to amplify germinal center output, which matters both for vaccine responses and for autoimmune antibody production. Regulatory T cells, meanwhile, produce dopamine to inhibit their own suppressive function in an autocrine loop, a bit like a brake that releases itself under certain conditions. Dendritic cells release dopamine during antigen presentation, preferentially steering T cell responses toward Th2 and Th17 subtypes, which is relevant to rheumatoid arthritis pathology. And in Parkinson’s disease, where dopaminergic neurons die, the loss of dopamine from immune cells may contribute to the neuroinflammatory environment in ways that are only now being considered.
GABA, the brain’s main inhibitory neurotransmitter, has generated perhaps the most striking recent finding in the field. A 2021 Nature paper showed that B cells in tumors produce GABA, which then induces macrophages to release IL-10, which in turn suppresses the cytotoxic function of CD8 T cells. In other words, B cell-derived GABA is actively protecting colorectal tumors from immune attack. When the GABA synthesis gene was knocked out specifically in B cells, CD8 T cell activity was restored and tumor control improved. That result immediately suggested a therapeutic target, though the same GABA signaling that suppresses anti-tumor immunity in the colon may have an entirely different function in, say, peritoneal macrophages or lymph node dendritic cells. Context, again, is everything.
The clinical potential here is real, if complicated. Clinical trials are already running on some of these pathways. Selective serotonin reuptake inhibitors (SSRIs), long used as antidepressants, have now been found to enhance the tumor-killing capacity of CD8 T cells by blocking a transporter that sequesters serotonin and suppresses cytotoxicity. Early data suggest SSRIs may synergize with immune checkpoint inhibitors, the drugs that have transformed cancer treatment over the past decade. Beta-blockers, which target adrenergic receptors, are being tested alongside anti-PD-1 antibodies in melanoma. Oral GABA supplementation has been studied in type 1 diabetes and rheumatoid arthritis. Vagus nerve stimulators implanted in RA patients have shown clinical improvement. The neuroimmune axis, once thought to be primarily about the nervous system signaling to the immune system, turns out to run bidirectionally, and the immune side of the conversation may offer more accessible pharmacological handles than anyone had expected.
What the review from the Hong Kong group makes clear is that the field is still in an early mapping phase. The tools for tracking neurotransmitter production in specific immune cell populations have only recently become adequate: reporter mouse strains expressing fluorescent proteins under the control of synthesis enzyme genes, cell-type-specific knockouts, real-time fluorescent probes that can visualize dopamine or norepinephrine being released from activated B cells. Single-cell RNA sequencing is beginning to reveal which immune subsets express which synthesis enzymes under which conditions. The picture that emerges is not simple. It is a system of remarkable local precision: short-lived molecules acting over microscopic distances, with effects that depend entirely on which receptors are present on neighboring cells, what other signals are in the microenvironment, and what the tissue itself needs at that moment.
There is a conceptual shift embedded in all of this that is worth sitting with. The immune and nervous systems have long been described as distinct physiological entities that communicate with each other, via cytokines, via nerve fiber innervation of lymphoid organs, via the adrenal glands. What the neurotransmitter-producing immune cell research suggests is something more intimate: that the immune system has, in effect, evolved its own internal nervous system, using the same molecular vocabulary but without the wires. The immune cell is not simply listening to neural signals; it is generating neural signals itself, managing local tissue environments through chemistry that would not look out of place in a synapse. “Harnessing the immune system’s intrinsic ‘neural language’ may offer new strategies for restoring homeostasis and achieving durable therapeutic benefit,” the review concludes. Whether those strategies arrive in five years or twenty depends on how quickly researchers can resolve the context-dependency problem: which neurotransmitter, from which cell, in which tissue, in which disease, does what. The question is unusually specific. The answers, when they come, are likely to be the same way.
DOI: 10.1007/s44466-026-00028-2
ScienceBlog.com has no paywalls, no sponsored content, and no agenda beyond getting the science right. Every story here is written to inform, not to impress an advertiser or push a point of view.
Good science journalism takes time — reading the papers, checking the claims, finding researchers who can put findings in context. We do that work because we think it matters.
If you find this site useful, consider supporting it with a donation. Even a few dollars a month helps keep the coverage independent and free for everyone.