Two radioactive tracers go into the same brain, five weeks apart. They are hunting the same thing: the tangled knots of tau protein that mark out Alzheimer’s disease from the dozens of other conditions that fog the ageing mind. Same person, same stage of disease, same machine humming around the skull. And yet the two scans disagree, sometimes wildly, about whether the tau is even there.
That disagreement is the unsettling heart of a study published this week in The Lancet by a team led from the University of Pittsburgh. It suggests that the answer to a question with enormous stakes, who has Alzheimer’s biology in their brain, can hinge on which chemical you reach for first.
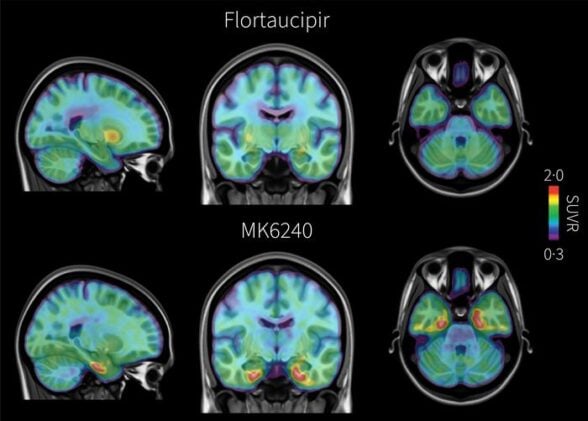
Here is the basic problem. Alzheimer’s has two molecular signatures: sticky amyloid-β plaques, which arrive early and often mean very little on their own, and tau tangles, which show up later and track much more tightly with the slide into dementia. Catch the tau and you have caught the thing that actually predicts decline. “Tau is the biology most closely tied to symptoms and future decline,” says Tharick Pascoal, a behavioral neurologist at Pitt and UPMC who led the work. To see it in a living brain, doctors use PET scans and a tracer, a compound that latches onto tau and lights up under the scanner.
For years the standard tracer in clinics across the US and Europe has been flortaucipir, sold as Tauvid. It is good at finding tau once the disease is well advanced and the tangles have spread out across the neocortex. Early on, in the medial temporal lobe where the trouble tends to start, it is less reliable.
So the Pittsburgh group ran what is, to their knowledge, the largest head-to-head tracer comparison yet attempted. They enrolled 775 people across eight sites in the United States and Canada; 682 made it through every procedure. Each one was scanned twice, once with flortaucipir and once with a newer investigational tracer called MK6240, the two scans falling inside a 45-day window so the disease itself had no real chance to move between them.
That tight window was the whole point. “Because participants received both tracer scans within a short window, we’re looking at the same moment in the disease course, so differences we see reflect the tracers, not changes over time,” says Guilherme Povala, a co-lead author.
The differences turned out to be substantial. MK6240 was simply better at telling Alzheimer’s-related impairment apart from impairment with other causes, with an area-under-the-curve score of 0.93 against flortaucipir’s 0.86, which sounds like a rounding error and is not. More striking was what happened among people who had no cognitive symptoms at all. In amyloid-positive volunteers who felt perfectly fine, MK6240 picked up tau in the medial temporal lobe more than twice as often: roughly 15 in every 100 versus 6. Run the maths and the newer tracer flagged 23 extra people per 100 as carrying early tau that flortaucipir had missed. Among people who already had memory problems, the gap held in the neocortex too, 28 percent positive versus 16, translating to 15 additional mild-impairment cases and 21 additional dementia cases per hundred scanned. And MK6240 reached its tau-positive threshold at a much lower amyloid burden, a Centiloid value around 53 rather than 81, meaning it caught the tangles earlier in the long, slow build-up.
None of this means flortaucipir is broken. The two tracers painted broadly the same map of where tau sits in the brain, and the older one carries something MK6240 does not yet have: years of post-mortem validation, the unglamorous business of checking scans against actual autopsied tissue. Flortaucipir is also the only tau tracer the FDA has approved for routine clinical use. MK6240, for now, lives in research labs and trials.
There is a wrinkle worth sitting with, too. The cohort was 93 percent White, which the authors flag plainly as a limit on how far the findings stretch. And a more sensitive tracer is a double-edged thing; finding tau earlier in someone who feels well is only useful if there is something to be done about it, or if the knowledge is wanted at all.
Still, the implications ripple outward fast. Tau PET is increasingly the gatekeeper for the new anti-amyloid drugs: the donanemab trial, for one, required a positive tau scan to get in the door. If the choice of tracer decides who counts as positive, then it quietly decides who qualifies for treatment, who gets enrolled in prevention trials, and who is told they are on an Alzheimer’s path. The study also found MK6240 tended to stage people about one Braak step further along, with more than a third of participants landing in a different stage depending on which scan you trusted. “People typically seek evaluation because they have memory concerns or other symptoms,” notes co-lead author Bruna Bellaver. Which tool meets them there is no longer a neutral technical detail.
Pascoal frames the stakes in terms of trajectory rather than diagnosis: detect tau earlier and stage it more precisely, he argues, and you can make better calls about who is truly heading toward Alzheimer’s, decisions that matter for trials now and for the clinic as new therapies arrive. The wider lesson may be quieter and more awkward. A decade of tau maps, drawn with a tracer we now know runs cautious, might have been telling us the disease starts later, and in fewer people, than it really does.
https://doi.org/10.1016/S0140-6736(26)00789-2
Frequently Asked Questions
Why does it matter which tau tracer a clinic uses?
Because the two tracers disagree about who has detectable tau. In this study the newer MK6240 flagged more than twice as many symptom-free people as carrying early tau, and staged many others further along the disease. Since tau scans now help decide who qualifies for anti-amyloid drugs and prevention trials, the tracer choice can quietly determine who gets access to treatment.
Is MK6240 available at my doctor’s office?
Not for routine care. MK6240 is still investigational and is used mainly in research and clinical trials. Flortaucipir, marketed as Tauvid, is the only tau PET tracer the FDA has approved for clinical use, so it remains the standard in US and European clinics for now.
Does a positive tau scan mean someone will definitely get dementia?
No. Tau tracks more closely with cognitive decline than amyloid does, but a positive scan signals risk and disease biology, not a certain outcome. Many people carry amyloid without progressing, and the long-term meaning of early tau picked up by a more sensitive tracer is still being worked out.
How can two scans of the same brain reach different answers?
The tracers bind tau tangles slightly differently and carry different background noise. MK6240 is more sensitive to early tangles in the medial temporal lobe and reaches a positive reading at lower amyloid levels, while the older flortaucipir is more prone to off-target signal and less reliable for early deposits. Same brain, different chemistry, different verdict.
ScienceBlog.com has no paywalls, no sponsored content, and no agenda beyond getting the science right. Every story here is written to inform, not to impress an advertiser or push a point of view.
Good science journalism takes time — reading the papers, checking the claims, finding researchers who can put findings in context. We do that work because we think it matters.
If you find this site useful, consider supporting it with a donation. Even a few dollars a month helps keep the coverage independent and free for everyone.