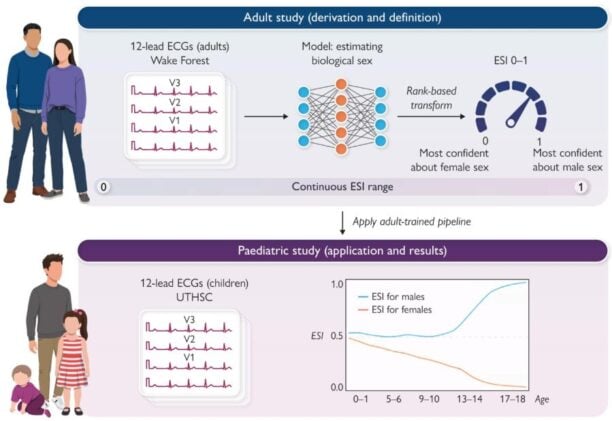
Feed enough heartbeats into an AI and it starts to see things clinicians have never thought to look for. That, in essence, is what happened when researchers at Wake Forest University School of Medicine pointed a neural network trained on adult hearts at 61,930 electrocardiograms from children as young as a few weeks old. The model, which had never seen a paediatric waveform during training, began sorting the ECGs not just by sex but by something more interesting: how far along each child was on the road toward adult biology. In infants the algorithm was almost guessing. In seventeen-year-olds it was nearly perfect.
The finding, published in European Heart Journal – Digital Health, suggests that the humble ECG, a test invented to catch electrical problems in the heart, may be quietly encoding the full arc of human development in its waveforms all along.
The electrocardiographic sex index, or ESI, was developed originally to capture something subtler than a binary label. Standard AI heart analysis tends to classify patients as male or female and stop there; ESI instead generates a continuous score from zero to one, with values near one reflecting ECG patterns typical of adult males and values near zero reflecting female patterns. In adults, the index had already demonstrated that people whose hearts “look” biologically inconsistent with their recorded sex face higher risks of heart failure and kidney disease, suggesting the signal is picking up genuine physiology rather than noise. But nobody had looked at what the same score does in children.
What it does, it turns out, is track puberty. With remarkable fidelity.
In early childhood, the ESI scores of boys and girls clustered around 0.5, meaning the algorithm could barely distinguish between them. Then, somewhere in late childhood, the scores started to pull apart. By mid-adolescence, boys’ scores were climbing steadily toward 1.0 while girls’ drifted toward 0.0, before plateauing roughly where adult values sit. The age at which divergence became pronounced maps closely onto the known biology of the hypothalamic-pituitary-gonadal axis, the hormonal cascade that sits dormant through most of childhood before switching back on at puberty.
“One of the most exciting aspects of this work is it shows routine ECG data may contain meaningful information about biological maturation in children and adolescents,” said Tolga Hayit, a computer scientist and visiting researcher at Wake Forest and the study’s co-lead author.
The practical significance of this might not be immediately obvious, so it’s worth dwelling on what paediatric researchers actually have to work with. Large datasets involving children routinely lack hormone measurements or Tanner staging (the standard five-stage clinical scale for assessing pubertal development), largely because collecting that data requires physical examination and specialist input that most studies can’t afford or access at scale. Researchers have long made do with sex as a simple binary covariate, which is, to put it mildly, a fairly rough approximation of what’s actually happening inside a developing body. An ECG-derived score that tracks maturation continuously could fill that gap considerably, and ECGs are already collected routinely in paediatric care for dozens of other reasons.
A Model That Learned Adults, Then Read Children
The methodological wrinkle here is that the ESI model was never retrained on paediatric data. The researchers applied the adult-trained algorithm directly to the children’s ECGs, essentially asking: can a model that learned what adult sex looks like electrophysiologically also read developmental stage in younger hearts? The answer appears to be yes, though with caveats. Accuracy (measured by area under the receiver operating characteristic curve, or AUC) started poor, at about 0.59 in infants under a year old, and climbed steadily to 0.97 in seventeen-to-eighteen-year-olds, by which point the model was performing nearly as well as it does on adults. The pattern held consistently across both White and Black children in the dataset, and crucially, ECG heart rate, which declines substantially across childhood, turned out to be essentially uncorrelated with ESI, ruling out the obvious confound that the model was simply noticing that younger kids have faster hearts.
Ibrahim Karabayir, assistant professor of cardiology at Wake Forest’s Centre for Artificial Intelligence Research and the study’s other co-first author, thinks the implications extend well beyond developmental biology. “ECGs, traditionally underutilized for capturing developmental biology, can now, when coupled with state-of-the-art AI approaches, highlight their potential to uncover patterns of maturation and cardiovascular development at scale,” he said.
One application his team has in mind is arguably the most clinically pressing. Children who receive cardiotoxic cancer treatments, including anthracyclines and chest-directed radiation, face elevated risks of cardiomyopathy and heart failure that can emerge years or even decades after treatment ends. The risk is thought to be larger when treatment occurs before the heart has fully matured. If ESI can quantify how “adult-like” a child’s cardiac electrophysiology is at the moment of treatment, it could, in principle, help stratify which patients need the most intensive long-term cardiac monitoring. That hypothesis hasn’t been tested yet, the paper is careful to say, and the current study establishes nothing about outcomes. But the biological logic is coherent enough that survivorship cohorts with serial ECGs are likely the obvious next step.
What the Heart Already Knows
The deeper implication is perhaps worth sitting with. Electrocardiograms have been around since 1901. For most of that time, clinicians have read them for arrhythmias, ischaemia, conduction defects, and not much else in the developmental domain. The idea that the same ten-second trace might also encode where a child sits on the continuum from infant to adult biology, detectable by a model that wasn’t even looking for it, is the kind of finding that tends to reframe what a technology is actually for. Tanner staging, the current standard, requires a trained examiner and an in-person visit; hormone assays require blood draws and specialised labs. Both generate point estimates that age poorly in longitudinal studies. A continuous ECG-derived maturity score that updates every time a routine heart trace is collected is something rather different in character.
There are real limitations to acknowledge. The paediatric cohort was clinical rather than population-based, so the children in it were already, by definition, sick enough to need heart monitoring, which may not represent the full developmental range. And the absence of Tanner staging or hormone data means the ESI trajectories can’t yet be anchored to specific pubertal milestones. Those are fixable gaps, the sort a well-designed follow-up study could address. What isn’t fixable is the basic premise, which is that the ECG has apparently been holding this information all along. Hayit put it plainly: ESI “offers a continuous measure that may help researchers account for developmental stage when Tanner staging or hormone data are not available.” Which, in most large paediatric datasets, is most of the time.
https://doi.org/10.1093/ehjdh/ztag058
Frequently Asked Questions
What is the electrocardiographic sex index and how is it different from a standard ECG reading?
A standard ECG reading looks for specific abnormalities like arrhythmias or signs of a heart attack. The electrocardiographic sex index is an AI-generated score, ranging from zero to one, that captures the overall pattern of electrical activity in the heart as it relates to biological sex. Rather than flagging a single feature, it summarises thousands of subtle waveform characteristics at once. The innovation here is that this score, developed in adults, also turns out to track how mature a child’s cardiovascular system is, essentially because the same hormonal changes that drive puberty also reshape the heart’s electrical signature.
Why can’t researchers just use hormone tests or physical exams to measure puberty in large studies?
They can in smaller, controlled settings, but large datasets involving tens of thousands of children rarely include hormone measurements or Tanner staging assessments. Both require physical examination by trained clinicians or specialised blood testing, neither of which is routinely captured in electronic health records or standard clinical archives. This forces most large paediatric studies to treat sex as a simple binary variable, which is a crude proxy for the gradual, stage-by-stage biology of development. ECGs, by contrast, are already collected routinely, meaning a maturity score derived from them could be extracted retrospectively from records that already exist.
Could this eventually be used in clinical practice for individual children, or is it only useful for research?
At this stage it’s primarily a research tool, and the authors are careful not to claim otherwise. The study establishes that the index tracks development at a population level but doesn’t yet show whether it predicts outcomes for individual patients. The most promising near-term clinical application is in childhood cancer care, where knowing how “adult-like” a child’s heart is at the time of cardiotoxic treatment could theoretically inform monitoring strategies. But that hypothesis needs testing in outcome-linked longitudinal studies before any clinical guidance could follow.
Why did the AI perform so poorly on infants compared to teenagers?
Because infants’ hearts really are less sex-differentiated, at least electrophysiologically. The hormonal axis that drives the divergence between male and female cardiac patterns is largely dormant in mid-childhood, only reactivating at puberty. In infancy there is a brief hormonal surge (sometimes called “mini-puberty”), but after that, the heart’s electrical patterns in boys and girls are genuinely similar. The model isn’t failing on infants; it’s accurately reflecting the biology. As sex hormones rise through adolescence, the divergence the model was trained to detect in adults begins to appear, and performance improves accordingly.
ScienceBlog.com has no paywalls, no sponsored content, and no agenda beyond getting the science right. Every story here is written to inform, not to impress an advertiser or push a point of view.
Good science journalism takes time — reading the papers, checking the claims, finding researchers who can put findings in context. We do that work because we think it matters.
If you find this site useful, consider supporting it with a donation. Even a few dollars a month helps keep the coverage independent and free for everyone.